

Evidence of harm in children caused by the vaccines
Evidence of harm in children caused by the vaccines
Dr. Robert Malone has asked me to help gather data for a paper he is preparing. I'm sending him everything I have, but you may have additional information.


He is looking for papers he can cite showing any of the following:
COVID-19 vaccines are not safe in children
The risk-benefit ratio is completely upside down for children.
More children will die from COVID-19 vaccines than will be saved
He already knows about:
the Kostov paper
the Toby Rogers risk-benefit analysis (my commentary; Toby’s analysis)
the fact that the 6 month Pfizer trial showed no death benefit whatsoever,
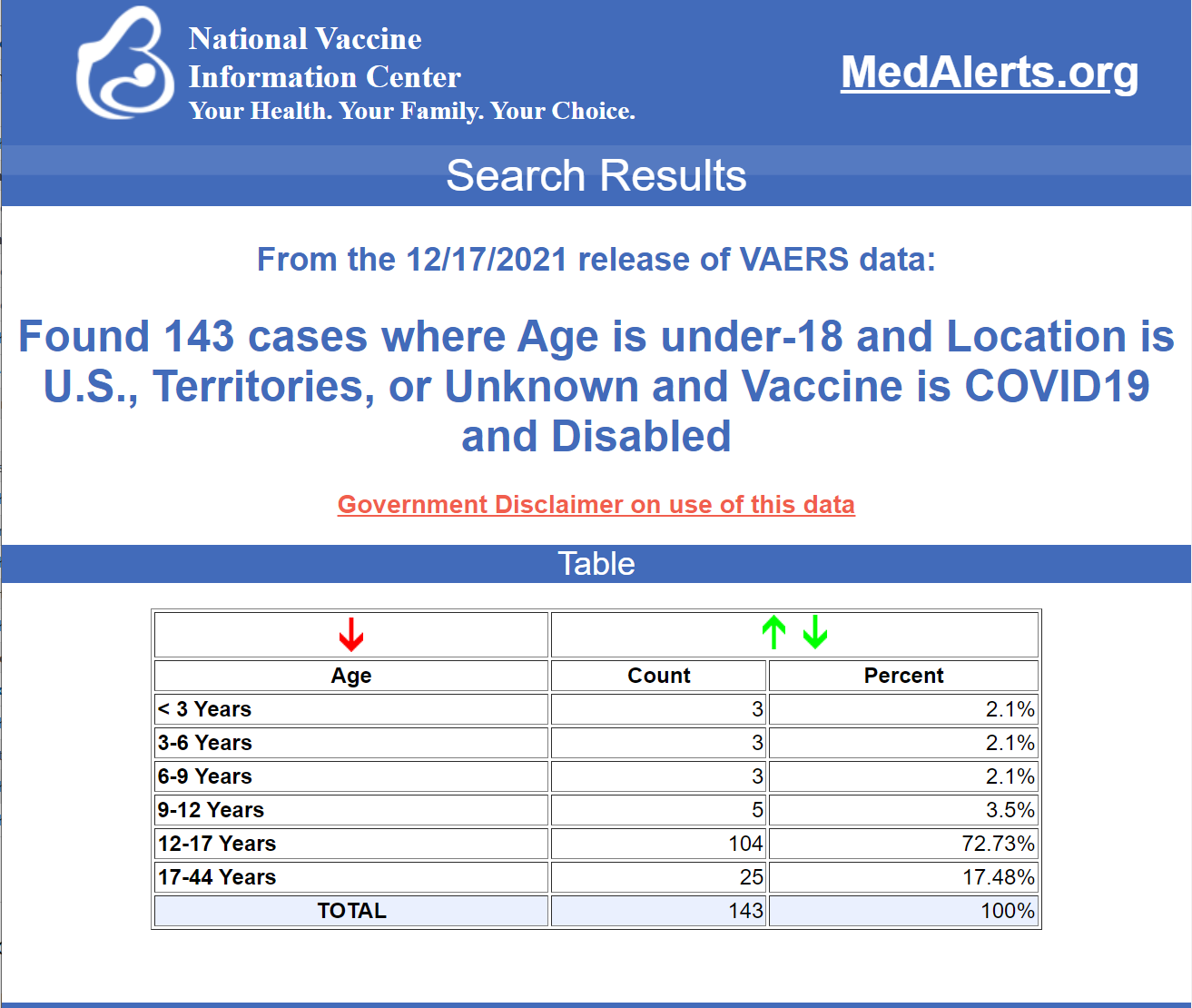
the latest VAERS data (search result below),
Myocarditis stats for kids with multiple anecdotes and more importantly, UCSF professor Vinay Prasad’s video showing the rate of myocarditis is higher from the vaccine than from COVID.
If you know of any similar sources in the peer reviewed literature or pre-print server (medrxiv, etc), please respond in the comments.
“Children” means 18 and younger.
He needs it today.
New articles suggested by readers
Association of Myocarditis With BNT162b2 Messenger RNA COVID-19 Vaccine in a Case Series of Children
https://jamanetwork.com/journals/jamacardiology/article-abstract/2783052
Cardiovascular magnetic resonance findings in young adult patients with acute myocarditis following mRNA COVID-19 vaccination: a case series
https://jcmr-online.biomedcentral.com/track/pdf/10.1186/s12968-021-00795-4.pdf
Possible Association Between COVID-19 Vaccine and Myocarditis: Clinical and CMR Findings
https://www.sciencedirect.com/science/article/pii/S1936878X2100485X?via%3Dihub
2 case studies here were 16 year old male and 17 YO female
The controversy surrounding vaccination of young people against COVID- 19
https://theexpose.uk/2021/10/28/child-deaths-62-percent-higher-since-covid-19-vaccination-began/
He needs to see Jessica Rose's long interview with Chris Masterjohn, PhD. Around the :56 minute mark she demonstrates the VAERS 5-11 children data and the UNDERREPORTING to the FDA committee by their medical adviser John Su.
Jessica Rose: VAERS, Myocarditis, COVID Vaccines, and So Much More |
1) SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis
https://doi.org/10.1101/2021.08.30.21262866
https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1
https://health-infobase.canada.ca/covid-19/vaccine-safety/#a4
3) More links here
https://drtrozzi.org/2021/12/28/vaers-mass-murder-update-and-sad-details-of-children-killed/
Dr. Trozzi has published a list of teenagers who died after the shot, taken from VAERS, that might serve the purpose.
SARS-CoV-2 mRNA Vaccination-Associated Myocarditis in Children Ages 12-17: A Stratified National Database Analysis
Preprint
https://www.medrxiv.org/content/10.1101/2021.08.30.21262866v1.full.pdf
There is the report made by Dr Jessica Rose and Dr Peter McCullough where they analyzed VAERS data of vaccination of children and that showed the harm and was peer-reviewed and published in all medial sites, but was suddenly removed 5 days prior FDAs decision on vaccinating children.
It's this one that she kept on her aubstack page:

Here are six studies that make the case for not vaccinating children:
1. A 2020 Yale University report indicates children and adults display very diverse and different immune system responses to SARS-CoV-2 infection which explains why they have far less illness or mortality from COVID.
According to the study:
“Since the earliest days of the COVID-19 outbreak, scientists have observed that children infected with the virus tend to fare much better than adults … researchers reported that levels of two immune system molecules — interleukin 17A (IL-17A), which helps mobilize immune system response during early infection, and interferon gamma (INF-g), which combats viral replication — were strongly linked to the age of the patients. The younger the patient, the higher the levels of IL-17A and INF-g, the analysis showed…these two molecules are part of the innate immune system, a more primitive, non-specific type of response activated early after infection.”
2. Studies by Ankit B. Patel and Dr. Supinda Bunyavanich show the virus uses the ACE 2 receptor to gain entry to the host cell, and the ACE 2 receptor has limited (less) expression and presence in the nasal epithelium in young children (potentially in upper respiratory airways).
This partly explains why children are less likely to be infected in the first place, or spread it to other children or adults, or even get severely ill. The biological molecular apparatus is simply not there in the nasopharynx of children. By bypassing this natural protection (limited nasal ACE 2 receptors in young children) and entering the shoulder deltoid, this could release the vaccine, its mRNA and LNP content (e.g. PEG), and generated spikes into the circulation that could then damage the endothelial lining of the blood vessels (vasculature) and cause severe allergic reactions (e.g., here, here, here, here, here).
3. William Briggs reported on the n=542 children who died (0-17 years (crude rate of 0.00007 per 100 and under 1 year old n=132, CDC data) since January 2020 with a diagnosis of COVID linked to their death. This does not indicate whether, as Johns Hopkins’ Dr. Marty Makary has been clamoring, the death was “causal or incidental.” That said, from January 2020, 1,043 children 0-17 have died of pneumonia.
Briggs reported:
“There is no good vaccine for pneumonia. But it could be avoided by keeping kids socially distanced from each other — permanently. If one death is “too many,” then you must not allow kids to be within contact of any human being who has a disease that may be passed to them, from which they may acquire pneumonia. They must also not be allowed in any car … in one year, just about 3,091 kids 0-17 died in car crashes (435 from 0-4, 847 from 5-14, and 30% of 6,031 from 15-24). Multiply these 3,000 deaths in cars by about 1.75, since the COVID deaths are over a 21-month period. That makes about 5,250 kids dying in car crashes in the same period — 10 times as many as Covid.”
Briggs concluded: “there exists no justification based on any available evidence for mandatory vaccines for kids.”
4. Weisberg and Farber et al. suggest (and building on research work by Kumar and Farber) that the reason children can more easily neutralize the virus is that their T cells are relatively naïve. They argue that since children’s T cells are mostly untrained, they can thus immunologically respond (optimally differentiate) more rapidly and nimbly to novel viruses such as SARS-CoV-2 for an effective robust response.
5. Research published in August 2021 by J. Loske deepens our understanding of this natural type biological/molecular protection even further by showing that “pre-activated (primed) antiviral innate immunity in the upper airways of children work to control early SARS-CoV-2 infection … the airway immune cells in children are primed for virus sensing…resulting in a stronger early innate antiviral response to SARS-CoV-2 infection than in adults.”
6. When one is vaccinated or becomes infected naturally, this drives the formation, tissue distribution and clonal evolution of B cells, which is key to encoding humoral immune memory.
Research published in May 2021 showed that blood examined from children retrieved prior to COVID-19 pandemic have memory B cells that can bind to SARS-CoV-2, suggestive of the potent role of early childhood exposure to common cold coronaviruses (coronaviruses). This is supported by Mateus et al. who reported on T cell memory to prior coronaviruses that cause the common cold (cross-reactivity/cross-protection).
There is no data or evidence or science to justify any of the COVID-19 injections in children. Can the content of these vaccines cross the blood-brain barrier in children? We don’t know because it wasn’t studied.
There is no proper safety data. The focus rather has to be on early treatment and testing (sero antibody or T-cell) to establish who is a credible candidate for these injections, as it is dangerous to layer inoculation on top of existing COVID-recovered, naturally acquired immunity.
There is no benefit and only potential harm/adverse effects (here, here, here).
Please respond in the comments if you have something useful.
Here’s the death data from VAERS. 38*41=1,558 deaths approximately from the vaccine
For disabled, there are 3.8 times as many as died. So 143*41=5,863 kids disabled. How does that compare with the number of teens disabled from COVID?
Soooo, I go to read the Kostov article and it’s been RETRACTED!! No reason given!🤬
… my 12 year old son asked the question’ Dad how many kids went to hospital with COVID?’ After I said good question , I said he could find out for himself on the NZ Ministry of Health COVID website. When the site came up, I asked him if he could see the data for 10-19 year olds, and asked him how many kids went to hospital. He read the data, and said “18. ‘ when he looked at the Medsafe Safety Alert graph showing 28 kids in the same age group had myocarditis after vaccine, my son said “ That’s bad , don’t do it. ( ie get a Pfizer injection). That’s more than the kids who went to hospital with COVID.”